
Cancer drug prices as high as a Ferrari… per year!

I am not suggesting that a car is worth more than a life. Far from that. The Hippocrates oath dictates helping everyone to the best of our abilities. But have we reached the point where cancer drug prices are irrational? The consensus is yes. Think about this: Medical costs are the number one reason for filing bankruptcy in the US. We can no longer turn a blind eye to a dangerous problem threatening many families. Everyone agrees that healthcare costs are ballooning and that radical change is needed. In oncology, one thing is certain though: Cancer drug prices have become prohibitive and gotten way out of control. But how did we get here?

Let’s start with a simple example. Using the car analogy in the title, a Ferrari is more expensive than a Prius. It is faster and made of superior elements. It is also rarer. Only 7,000 cars a year compared to 1.7 million Prius a year. The combination of rarity, technical prowess and the feeling of importance it gives its owners justify the price tag.
As individuals, we intuitively understand the laws of supply and demand market and price commodities differently depending on their perceived value. In extension to drug pricing, you would be justified to think that the most effective cancer drugs are priced in a similar fashion. But they are not. In fact, the pricing of cancer medications has little to do with the laws of supply and demand and operates on the principle of “what the market can tolerate”. Simply put, rather than compete with each other, pharmaceutical companies have a tacit agreement that they will keep prices comparable yet very high with the understanding that patients and payers have no choice but to pay. Rather than compete to lower prices, they effectively are in agreement to increase prices.
I-But patients cannot afford the ever rising cancer drug costs
In 2015, 1.7 million new cases of cancer were diagnosed. Aside from the minority of patients with early stage cancer who can be cured by surgery or radiation alone, most patients will require prescription drugs.
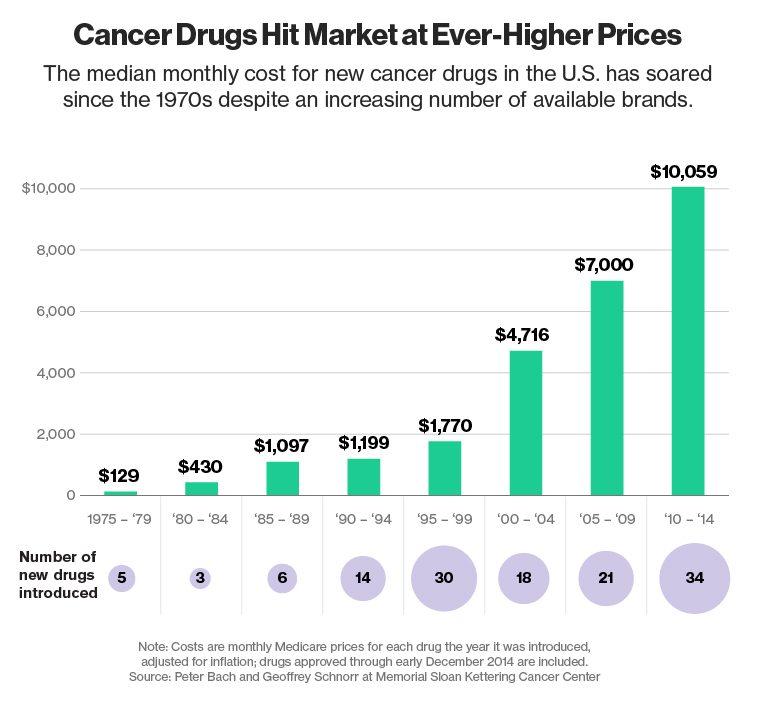
Those drugs are expensive. Very expensive. In fact, the cost of cancer medications has increased exponentially over the last 15 years. The cost of one year’s worth of cancer drugs has increased from less than $10,000 prior to 2000 to more than $100,000 by 2012. This is despite a decrease of eight percent in household income during that time.
This dramatic cancer drug cost increase is not without consequences. According to Dr Kantarjian who heads the Leukemia department at the MD Anderson Cancer Center in Houston, TX, 10-20% of cancer patients either forfeit treatment or resort to a suboptimal treatment due to financial reasons. He has spearheaded the effort to reduce drug costs over the last few years.
II-Common industry trends:
Those practices are not isolated to cancer treatments, as Valeant Pharmaceuticals  and Turing Pharmaceuticals have shown us over the last few months. In the case of the well publicized case of Turing Pharmaceuticals, the price of Daraprim was increased by 5,000%. Valeant was following similar practices by buying drugs then raising their prices, on average, 66 percent. Although Valeant announced plans to reorganize few days ago (and as of yesterday facing criminal investigation), whether this will affect drug prices remains to be seen.
and Turing Pharmaceuticals have shown us over the last few months. In the case of the well publicized case of Turing Pharmaceuticals, the price of Daraprim was increased by 5,000%. Valeant was following similar practices by buying drugs then raising their prices, on average, 66 percent. Although Valeant announced plans to reorganize few days ago (and as of yesterday facing criminal investigation), whether this will affect drug prices remains to be seen.
III-So how are the prices determined? And why our hands have been tied.
In a CBS News interview in October 2014, Dr. Peter Bach of Memorial Sloan Kettering Cancer Center, explained how drug companies set the prices of the drugs they place on the market: “We have a pricing system for drugs which is completely dictated by the people who are making the drugs. It’s corporate Chuptzah” It’s an arbitrary number the companies making the drugs determine. In simple terms, the prices are set depending on “how brave [the companies] are and how little they want to end up in the New York Times or on 60 Minutes.“
While one could make the argument that newer medications should be more expensive, one would also expect that older medications would depreciate as development costs are amortized and competitor drugs enter the market. However, this is not the case. Even after new drugs have come onto the market (generics and competitor drugs), many companies continue to raise costs on existing drugs. For example, the blood cancer drug Gleevec (also marketed internationally as Glivec) has gone from ~ $3,000 a year in 2001 to $146,000 in 2016 despite competition in the marketplace.

You would assume that Medicare, with its large coverage and clout could negotiate better deals. However, Medicare cannot negotiate with drug companies by law. As difficult it is to understand and harder to believe, this means that Medicare is held hostage to the prices set by the companies. More on this below.
Since patients are required to pay for 20 percent of the cancer drug costs out of pocket, costs become, quite simply, unsustainable for most of the patients being treated for cancer. For example, when Memorial Sloan Kettering refused to dispense Zaltrap because of its cost, Medicare patients would have been required to pay $2,000 in monthly co-pay, the equivalent of their entire monthly income. Not to mention that the 42 day benefit offered by Zaltrap would cost $60,000.
We have a pricing system for drugs which is completely dictated by the people who are making the drugs. It’s corporate Chuptzah” It’s an arbitrary number the companies making the drugs determine. In simple terms, the prices are set depending on “how brave [the companies] are and how little they want to end up in the New York Times or on 60 Minutes.“ Peter Bach, MD
IV-How does Big Pharma Justify these Prices?
In the wake of the recent reports about Turing and Valeant, other pharmaceutical companies have distanced themselves from these practices. To justify the ever rising cancer drug prices, they cite several reasons including the high cost of research and development and that controlling prices would hinder competition. Dr Kantarjian explores all these reasons in the Mayo Clinic Proceedings

1-Drugs are expensive to develop (But who is really Footing the Bill?)
Over the years, the price tag of 1 billion dollars per drug that makes it to the market has been repeatedly floated. Per Andrew Witty, the chief executive officer (CEO) of GlaxoSmithKline, the $1 billion cost is “one of the great myths of the industry.” The real research cost of a drug stands to be a tenth of this amount, with marketing budgets added in the “cost” of drug development.
Even more surprising is the claim that record profits are needed in order to fund research. A closer look shows that the majority of drug research is funded by various governmental agencies. In the case of specific cancers, such as breast cancer, prostate cancer, and other high profile cancers, a fair amount of charitable contributions are made to help fund research as well.
“The $1 billion cost is one of the great myths of the industry.” Andrew Witty, CEO of GlaxoSmithKline
2-Higher prices are needed because of price caps in other countries
Drug makers claim that U.S. markets are bearing the brunt of the costs for researching these drugs. But there is no reason that the U.S. alone should be responsible for the burden of costs for researching drugs that benefit the entire world, reports FiercePharma, particularly when our GDP is not really higher than that of European countries that enjoy much lower rates.
Their final justifications, though, come in reporting about high survivability rates in the U.S. compared to other countries as proof that the U.S. market can support those high prices. That argument fails to take into account the toll these prices are taking on taxpayers and families alike. Meanwhile in Europe, the government has taken action to cap most drug prices and even drive some down.
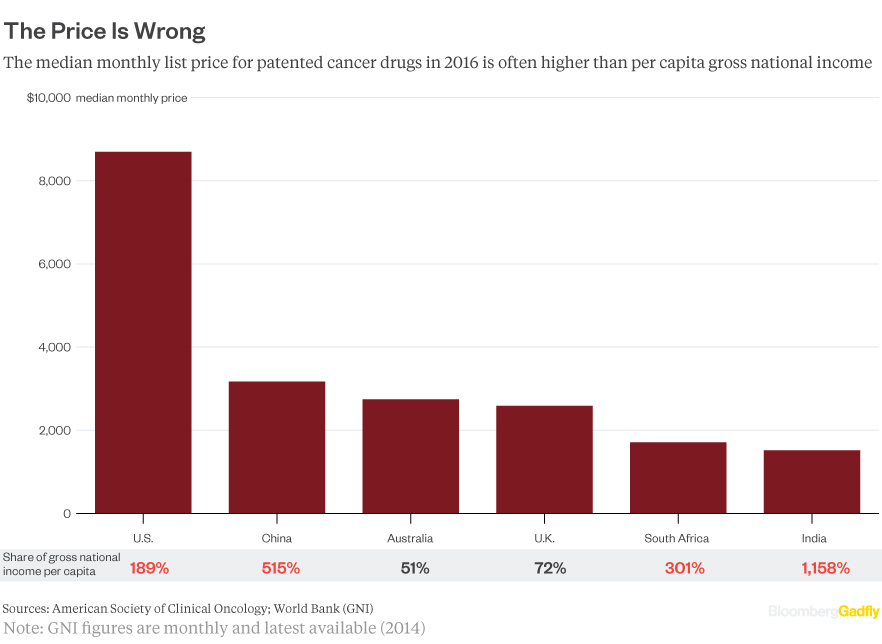
V- How do U.S. Drug Prices Compare to the Rest of the World?
The Insurance Journal compared U.S. drug prices to those in other countries. As of 2014 when the study was conducted, U.S. drug prices were three times higher than those in Britain, six times higher than those in Brazil, and 16 times higher than drug prices in India.
An illustration of some extreme example is the cancer drug Gleevec. Gleevec is used to treat leukemia and costs $159 for a year’s worth of treatment in India compared to $106,000 in the U.S., according to Huffington Post. Other examples cited for their massive price differences are the lung cancer drug Tarceva ringing in at $236 compared to $79,000 in the U.S. and Tykerb which costs $4,000 in India compared to U.S. prices which are $70,000 greater.
The report in Insurance Journal goes on to say that between 2008 and 2014, U.S. drug prices for top brand-name drugs increased by 127 percent compared with price increases of only 11 percent, during that six year period, for common household goods.
VI-What is the Role of Medicare?
Unfortunately, the hands of Medicare are tied when it comes to affecting cancer drug prices. The law that created Medicare Part D is the same law that denies the government to negotiate on behalf of recipients for lower costs.
The law that created Medicare Part D fed millions of new customers to the pharmaceutical companies and then tied to the hands of the government to negotiate on behalf of these new customers, many of whom are being crippled by the high costs of medications needed.
How big is the problem of non-negotiation for drug prices in Medicare Part D? The Wall Street Journal (WSJ) reports that the government could save between $15.2 and $16 billion per year if Medicare was able to negotiate for the same prices Medicaid and the Veterans Benefits Administration (VBA) pay for medications. Current reports cited in the WSJ article indicate that Medicare currently pays 80 percent more than VBA for brand name drugs and 73 percent more than Medicaid.
One thing that has been noted is that as the cancer drug prices are increasing, so is the spending of drug companies on their lobbying efforts. In fact, the first quarter of 2014 saw five pharmaceutical giants reporting million dollar increases on their federal lobbying efforts – the same companies who claim that cutting their fees to Medicare will cause them to limit their efforts to research and develop new drugs.
VII- First, do no harm. Financial toxicity is harm
Current cancer patients are suffering in many ways from the current price gouging that appears to be taking place. They are being informed that they must take these drugs or die prematurely, and then given price tags they know they cannot pay.

cancer drug
Desperate people make desperate decisions in the hopes of buying more time. Days, weeks, months, and years. And the costs devastate the families, robbing children of college funds, parents of retirement funds, and causing bankruptcies.
NerdWallet reports that 1.7 million Americans are living in households that will be forced to declare bankruptcy due to their inability to pay for their medical bills.
Many believed the affordable care act would prevent many of bankruptcies related to medical bills. The startling truth is that 78 percent of people who claim bankruptcy due to medical bills have insurance.
The problem is that insurance is not the solution. Most insurance companies will exclude cancer treatments they feel are new or experimental. Then there are limits for how much insurance companies will pay out for certain treatments and some policies have a lifetime limit on coverage. Then there are deductibles, copayments, gaps in coverage, and services that are simply not covered.
People who are really sick for a long period of time will even lose their jobs and the precious insurance coverage that job provided.
Keep in mind that there are other costs related to treatment and illness that go beyond the medications alone, such as:
- Child Care
- Transportation
- Lost Wages
- Partner’s Lost Wages
And more…. All of this can really level a family’s careful financial planning. Those that don’t have any sort of safety net to help cover the costs of treatment and absences from work face even faster financial ruin.
The final result is that 62.1 percent of all bankruptcies filed in the U.S. are the result of medical expenses. Medical expenses are the most common reason for bankruptcy in the US.
The other side of the coin is sadder still. Novant Health reports that nearly eight percent of US adults simply do not fill their prescriptions for life saving drugs because they can’t afford them.
This is in addition to the 25 million adults who do not take their prescriptions as indicated, skip doses, take less medicine than prescribed by splitting pills or taking them every other day, and delay refills to cut costs.
In a different report by NPR, an estimated 10 to 20 percent of cancer patients are compromising their prescribed treatments if not skipping them altogether because of the treatment costs. NPR explains that launch prices of new treatments are increasing by an average of $8,500 per year prompting many patients to take this drastic action.
VIII-What can Oncologists do about the Problem?

Previously, physicians tried to avoid the debate of price versus benefits when dealing with the lives of their patients. How do you put a price on a life? But the costs of newer medications have caused many to reassess how they are approaching prescribing new medications for their patients. Some physicians are discussing options with their patients and taking a more active role in explaining the finances of cancer treatments.
In a first at the time and as mentioned above, Memorial Sloan Kettering rejected Zaltrap based on their prices alone. They determined that the new drugs do not offer an adequate improvement over existing drugs to warrant their outrageous price tags.
Some oncologists are lobbying for congressional action that will prevent companies that make cancer treatments from delaying generic companies from entering the market as they have been doing in the past. Another change, they are calling for, according to NPR is the creation of a committee that would review new cancer drugs entering the market and propose fair prices based on the benefits these drugs bring to the table.
Dr. Kantarjian has stated that the high cancer drug cost is actually harming the cancer patients he treats. At the time of a 2013 statement, the focus was on the high costs of leukemia treatments. Since then, the focus has shifted to all forms of cancer and doctors are speaking out more frequently on the topic.
Another thorny topic among oncologists is the issue of reimbursement. When a chemotherapy drug is administered, the clinic charges 6% of the price of the drug as an infusion fee. This has led to instances of conflict of interest whereby oncologists choose the more expensive cancer drug that would be more lucrative to the clinic. Uncoupling the infusion fee from the price of the cancer drug would decrease the likelihood of oncologists administering a drug solely because of its price.
IX- Proposed solutions
The proposed solutions vary from the practical to the ambitious. Dr Ayalew Tefferi, a prominent oncologist at the Mayo Clinic suggested that patients get their medications from Canada. In an editorial article for the Mayo Clinic proceedings, he led 118 oncologists in asking for a new regulatory body to set the prices of new approved. They also urged to allow cheaper drugs to be imported from other countries such as Canada.

Dr. Kantarjian proposed a new system for pricing medications that will literally force new medications entering the market to “sing for their supper” so to speak. His proposal involves pricing medications according to the benefit they present to patients.
Citing the fact that the high costs of cancer treatments were causing economic and emotional harm to cancer patients who are often forced to choose between their lives and the financial security of their families, he has proposes a system that would end this type of “medical Darwinism” where only the financially fittest, those who could pay for the treatment would live.
After all, cancer drug company cost estimates do not account for donations, charitable gifts, government grants, and other funding received from private sources to fund research for treatments and the search for cures. He states that 85 percent of the cost of basic research is funded by taxpayers.
In an editorial in Blood, he led 120 oncologists in requesting better pricing practices and in asking for a shift of focus to higher payments for drugs that add years to the lives of their patients rather than those that only add a few weeks.
While widespread solutions haven’t presented themselves as of yet, it appears that doctors are left to counsel patients about options and look for treatments that will provide the best possible treatment for their patients’ physical and economic health.
In conclusion, there appears to be an increased awareness about the toll cancer drug prices are taking on American families. While no immediate solution has been implemented, an increased media exposure and physician awareness could be the harbor of a fairer pricing value system in the near future.
Latest posts by Michel Choueiri (see all)
- Does cancer smell? Can people smell cancer? - September 28, 2016
- Does Cancer Itch? Which cancers cause itching? - August 19, 2016
- Cancer drug prices as high as a Ferrari… per year! - August 16, 2016